Oralchirurgie 26.08.2016
Die follikuläre Zyste – Schwierigkeiten bei der präoperativen Röntgendiagnostik

share

Die klinische Differenzierung eines dentalen Follikels von einer dentogenen Zyste anhand eines Röntgenbildes wird kontrovers diskutiert. Die folgende Studie beschäftigt sich mit den Schwierigkeiten der Diagnose, den geschlechtsspezifischen Unterschieden und der regionären Auftrittshäufigkeit dentogener Zysten.
Abstract
Ziel dieser Studie war es, erstens die radiologische Diagnose eines dentalen Follikels oder einer dentogenen Zyste mit der Histologie des perikoronalen Gewebes zu vergleichen. Zweitens war es das Anliegen der Studie, einen geschlechtsspezifischen Unterschied im Auftreten der dentogenen Zysten und drittens die Region des gehäuften Auftretens für dentogene Zysten festzustellen. Die klinische Diagnose eines hyperplastischen oder erweiterten Follikels sowie einer dentogenen Zyste basierte auf der Betrachtung der Größe der perikoronalen Transluzenz von etwa 3.427 retinierten oder impaktierten unteren und oberen dritten Molaren.
Das perikoronale Gewebe wurde nachträglich zur histologischen Untersuchung gesandt, um eine exakte Diagnose zu erhalten. Sowohl das Alter der Patienten als auch die Lokalisation wurden erfasst.14,44 % der klinisch als dentale Follikel diagnostizierten Fälle waren dentogene Zysten im Frühstadium, und weitere 8,1 % wurden als voll ausgebildete dentogene Zysten durch die Histologie ausgewiesen. Das Patientenalter für beide Läsionstypen war im Wesentlichen gleich. Vergrößerte dentale Follikel und frühe sowie ausgebildete dentogene Zysten fanden sich vorwiegend im Bereich der dritten Molaren im Unterkiefer links. Beide Läsionstypen traten mehrheitlich bei Frauen auf. Aufgrund der Tatsache, dass klinisch nicht zwischen einem dentalen Follikel und einer dentogenen Zyste anhand eines Röntgenbildes unterschieden werden kann, sollte jedes perikoronale Gewebe, welches retinierte oder impaktierte dritte Molaren umgibt, zur histologischen Untersuchung eingereicht werden. Im Falle einer positiven Diagnose, einer dentogenen Zyste, sollten alle noch verbliebenen, retinierten und verlagerten dritten Molaren prophylaktisch entfernt werden.
Introduction
The dentigerous cyst is an odontogenic epithelial lesion that forms around the crown of an unerupted tooth. It develops from the dental follicular tissues by the accumulation of fluid between the inner enamel epithelium and the tooth crown, forming a cyst that surrounds the crown of the tooth and enlarges due to osmotic pressure.1–3 The reduced enamel epithelium undergoes metaplasia and can vary in thickness throughout the cyst. It is thought that inflammation is partially responsible for the pathogenesis of this cyst.
The distinction between the radiographic image of hyperplastic pericoronal follicular tissue and a small dentigerous cyst is controversial. Daley and Wysocki, in their comparative study of 1,662 dentigerous cysts and 824 dental follicles, showed considerable overlap in age distribution and site predilection.4 They concluded that reliably distinguishing between a small dentigerous cyst and an enlarged dental follicle may only be resolved by identifying a cyst cavity at surgical operation.
The radiographic appearance of the normal follicular tissue space has been regarded as varying from 2 to 5 mm in diametre.5,6 However, a subsequent study by Ahlqwist and Grondahl suggested that the normal follicular tissue space ranges from 3 to 4 mm.7 Damante and Fleury undertook a study to verify the relationship between the radiographically measured width of the pericoronal space and the microscopic features of the dental follicle in order to contribute to the differential diagnosis between small dentigerous cysts and hyperplastic follicular tissue.8 A trend was noted between the presence of inflammation and enlargement of the pericoronal space in partially erupted teeth and possibly in completely unerupted teeth. Curran et al. reported that in a sample of 2,646 pericoronal lesions 67 % were normal dental follicles and 28.4 % were dentigerous cysts.9
Despite the previous studies, the radiographic distinction between a normal follicular space and an early or fully formed dentigerous cyst is still not clear. The aims of this study were first to compare the radiographic diagnosis of an enlarged dental follicle and a dentigerous cyst with the histology of the pericoronal tissues in a large series of 3,427 surgically removed third molars, second to determine if there is a gender difference in the occurrence of dentigerous cysts, and third to determine the most common locations for such cysts.
Materials and Methods
This retrospective study was reviewed and approved by the University of Cape Town Department of Surgery Research Committee. The department follows the Helsinki Declaration. This was PROJECT 2006/20 and approved on 13 April 2006.
All reports of the histological findings as well as the original patient records from the practice were available for analysis. Patients were not identified by means of theatre records and data was obtained from actual patient files and subsequent histological diagnoses made.
Patients who had a removal of symptomatic unerupted or impacted mandibular and maxillary third molars in the author’s private oral and maxillofacial surgery practice over a period of 20 years were included in this study. All of the patients had preoperative panoramic radiographs. Prior to surgery, the radiolucent space associated with the tooth was assessed visually on the panoramic radiograph and a tentative clinical diagnosis of an enlarged follicle, or dentigerous cyst was made based on the perceived size of the space. Age and gender of the patient and location of the lesion were recorded. The 3,427 third molars and their associated pericoronal soft tissues were then submitted for microscopic analysis by an oral pathologist.
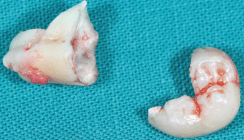
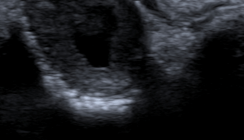
A hyperplastic dental follicle was diagnosed histologically when the soft tissue lining was composed of reduced enamel epithelium and there was an increased thickness of the follicular connective tissues, often containing numerous islands of odontogenic epithelium (Fig. 1). A cyst was diagnosed when there was metaplastic transformation of the reduced enamel epithelium of the follicle to a stratified squamous epithelium lining (Fig. 2). A chronic inflammatory cell infiltrate in the adjacent fibro-vascular connective tissues was a common finding (Fig. 3).
Results
Histologically, 1,071 (31.25 %) cases were diagnosed as hyperplastic follicles out of the 3,427 specimens evaluated. There were 495 (14.44 %) cases diagnosed as early dentigerous cysts, of which 84 (16.97 %) cases were found to be multiple early dentigerous cysts. There were 278 (8.11 %) fully formed dentigerous cysts. This totals 773 (22.55 %) cases of dentigerous cyst formation.
Hyperplastic follicles
Age
The age range for the histologically diagnosed hyperplastic follicles was between 14 and 46 years, with the largest number of cases between 14 and 21 years (Table 1). This was followed by a decreasing number to 36 years of age and thereafter there was a very small number of cases up to 46 years of age.
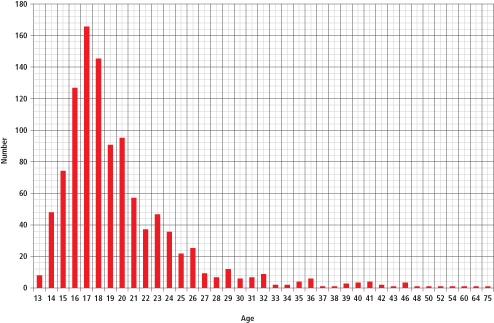
Table 1: Hyperplastic Follicular Tissue (n=1071)
Gender and site
The largest numbers of hyperplastic follicles, 294 cases (27.45 %), were located in the mandibular left third molar region, of which 97 cases were in males and 197 in females. This was followed by 290 cases (27.09 %) on the lower right side, 100 cases in males and 190 in females. In the maxilla, there were 219 (20.45 %) hyperplastic follicles on the upper right side, 79 in males and 140 in females, and 268 cases (25.02 %) on the upper left, which consisted of 74 in male patients, and 194 in females (Table 2).
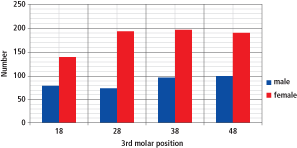
Table 2: Hyperplastic Follicular Tissue (n=1071)
Dentigerous cysts
Age
The age range for patients with dentigerous cysts was between 14 and 64 years with the largest number of cases at 21 years of age. There was a second increase in incidence at 26 to 28 years of age (Table 3). Thereafter there were only a very small number of cases from 30 to 64 years of age.
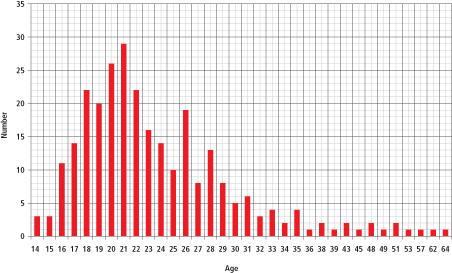
Table 3: Dentigerous Cyst (n=278)
Gender and site
Both female and male patients had similar numbers of dentigerous cysts in all locations (Table 4). The greatest number of cases occurred in the lower right with 58 in females (22.48 %) and 51 in males (18.34 %). On the lower left, there were 52 cases (18.71 %) in females and 44 (15.83 %) in male patients. On the upper right, there were 19 cases (6.83 %) in females and 20 cases (7.19 %) in males and on the upper left there were 21 (7.55 %) cysts in females and 13 (4.68 %) cysts in males.
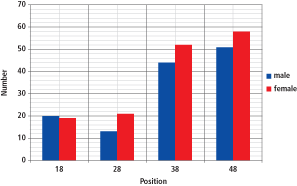
Table 4: Dentigerous Cyst (n=278)
Discussion
Shear and Speight have indicated that dentigerous cysts comprise 17.1 % of all jaw cysts. Our study showed a 14.44 % incidence of early dentigerous cysts and 8.11 % of fully formed dentigerous cysts in the third-molar regions.3 If the incidence of fully formed dentigerous cysts is combined with early dentigerous cysts, an occurrence of 22.55 % is obtained. This is more in keeping with the results published by Daley et al., where dentigerous cysts comprised 24 % of all jaw cysts and those of Jones et al. who showed an 18.1 % incidence of dentigerous cysts in a series of 7,121 odontogenic cysts.5,10
It is commonly understood that hyperplastic follicles have a pericoronal radiolucency of 4 to 7 mm, while dentigerous cysts have a pericoronal radiolucency of 6 to 9 mm. Therefore, by examining the radiographic image of third-molar pericoronal radiolucency, it is likely that a dentigerous cyst may be missed by the surgeon.
Although it is not cost effective to send all pericoronal tissues for microscopic examination, this should be done when the follicle is abnormally enlarged or if the tissue appears exceptionally thickened. It is also suggested that oral and maxillofacial surgeons or dentists be advised to monitor the postoperative healing of the surgical sites in their subsequent routine radiographic examinations of the patient. Moreover, because of the potential that an enlarged dental follicle around an impacted third molar may be pathologic, it is advisable that all impacted third molars be considered potentially pathologic, as noted in the position paper of the American Association of Oral and Maxillofacial Surgeons. Moreover, if one tooth shows an abnormally enlarged follicle, all non-functional third molars should probably be removed.11
Conclusions
Although the incidence of dentigerous cysts does not justify sending all associated dental follicles for microscopic examination, teeth with follicular enlargement should be removed. When the removal of one impacted third molar is indicated because of an enlarged follicle, it is advisable that the remaining impacted third molar teeth also should be removed.
Acknowledgements
The authors would like to acknowledge the help of Rafael Berezowski in the preparation of various graphs and his invaluable computer assistance in this paper. The authors would like to thank Dr. Horst Luckey most sincerely for the German translation of the abstract.
Hier geht es zur Literaturliste
Co-Autoren: Vincent M. Philips, BDS, PhD, DSc; Daniel M. Laskin, DDS, MS